David Mantik argues (in 'Murder In Dealey Plaza' XXXX) 1) that the Harper fragment is (mostly) occipital bone 2) that autopsy photo # 44 - otherwise known as 'F8' - shows the (outer) rear of JFK's skull. & 3) that the Harper fragment fits neatly into a vacancy in the rear skull seen in that photograph.
Mantik writes:
" At 5:30 pm, Saturday, November 23, a pre-med student, Billy Harper, found a fragment
of skull bone (7HSCAI23-124) on the grass south of Elm Street, not too far from where Jean Hill had been standing.
(The exact site is not well defined, however.) "
[In fact Harper subsequently marked the spot on a map :
See where Harper himself says he found it, well in front of the Presidential limousine.
See what is probably the Harper fragment leaving the skull in the Z film ]
Mantik takes up the story::
"Harper took it to his uncle, Jack C. Harper, M.D., who in turn showed it to A.B.
Cairns, the chief pathologist at Methodist Hospital. A total of three Dallas pathologists examined the bone and
they identified the site of origin as the occiput. (On 22 November 1992, on a Palm Springs radio talk show, I helped
to interview one of these pathologists, Dr. Gerhard Noteboom, who reaffirmed that conclusion; he also recalled
the lead deposit on the fragment.) The bone was then shipped to Admiral Burkley, who, in turn, gave it to the FBI,
where it was lost. Fortunately, photographs were taken in Dallas (Here). A ruler on the photograph permits an estimate of size: it is about 7 x 5.5 cm, and trapezoidal
in shape.
Joe Riley, Ph.D., a neuroanatomist (formerly in academia), places this bone into the parietal area (Joe Riley,
"Anatomy of the Harper Fragment," JFK Deep Politics Quarterly, April 1996).
See Riley's paper on the subject
Riley says, in a nutshell:
"The anatomical features of the Harper fragment demonstrate conclusively that it cannot be occipital bone."
Mantik:
"... as I continued to review the X-rays, the mystery photograph F8.. the statements of the Dallas pathologists and the Bethesda pathologists, and the fragment itself, I remained convinced that it was (mostly) of occipital origin. I believe that Riley has overlooked much valuable evidence, and that his objections can be effectively countered. The employment of the X-rays and the proper orientation of F8 are a powerful combination that should not be overlooked, especially when coupled with information on the bone itself."
Mantik's suggested placement of the fragment in the autopsy photo.
Mantik:
".. Both Angel [J. Lawrence Angel, Curator of Physical Anthropology at the Smithsonian,
who was consulted by the HSCA] and Riley argued for a parietal site based on the vascular grooves (curvilinear
indentations) and the foramina (perforating holes for small vessels) on the inside surface. But I found it easy
to demonstrate exactly these same features in the upper occipital bone on two genuine human skulls that I owned,
and I could easily see them in multiple anatomy textbooks, extending over many decades, so I did not consider these
arguments to be decisive."
Mantik does not produce any pictorial evidence to support this. I have not been able to find any. What I have been able to find supports Riley & Angel:
see a very interesting 'occipital'
QuickTime movie
Mantik:
"Moreover, the direction of the vascular grooves, although consistent with a parietal site, was also surprisingly consistent with an upper occipital site, which was also not hard to demonstrate. I could easily see these on my skulls (the grooves did go in the right direction) and it was not hard to find photographs in texts that were equally supportive. (I doubt that Angel ever did this exercise, since he automatically ruled out the back of the head, nor do I really know if Riley performed this exercise for the upper occiput, since he seemed so focused on the lower occiput.)"
Again we have to take Dr Mantik's word on this. And again, the evidence I have been able to find does not support him:
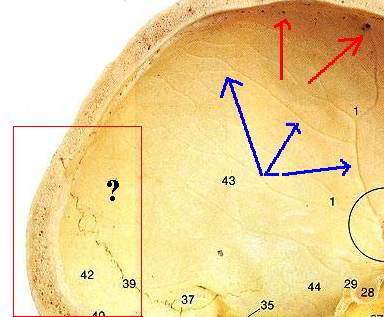
Note the deep vascular grooves (blue arrows) and the foramina (red arrows) around Angels' location for the fragment,
Mantik:
When I examined The triangular area of missing bone (see the small white triangle
in the figure in the Postscript), near the low midline, on photo F8, I remembered that I had.seen this empty triangle
before on the X-rays. (Although I did not mention it in the Postscript, this argument, too, helped to persuade
me of the correct orientation of F8.) I already knew, from naked eye viewing (with very myopic eyes, the best kind
for the job) and from detailed OD measurements, that bone was absent in just this same triangular area on the frontal
X-ray (approximately inside the lower left nose). I had not gone looking for this; I merely happened one day to
notice it while at the Archives. Since no one had reported such missing bone from the left; side of the skull,
I was surprised and decided to explore it further with more OD measurements. Since I now knew the orientation of
F8 and its dimensions (there is a ruler on F8) and because I could correlate identical objects on F8 with the photographs
and because I already knew the dimensions on the skull (from my own measurements at the Archives), I could now
estimate the size of this empty triangle on F8.
It was probably some time later, however when I returned to this jigsaw puzzle, trying to imagine where the Harper
fragment might fit into the skull. When I did, I realized that its left edge (on the exterior view) might fit into
the empty triangle. In fact, it seemed to fit extremely well, so I proceeded to the other borders.
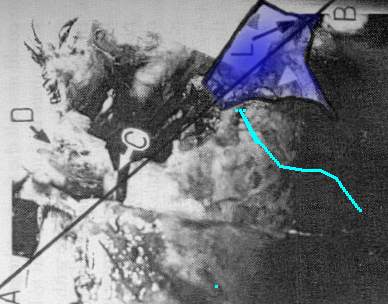
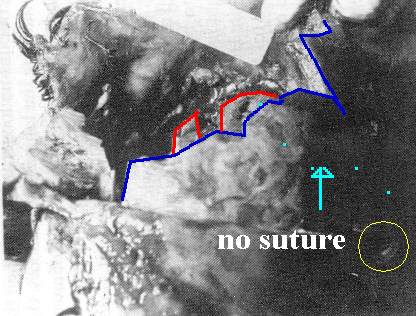 F8 (above) shows the distant bone in focus & the nearby material out of focus. The blue line shows the border of the 'near' area, the red line shows the sharply focussed 'distant' bone margins. Mantik (right) fits the Harper frag (at it's near edge) to a combination of both 'near' & 'far' bone structures - in essence, to a non existent line. Also we would expect to find lamboid suture along the blue lines (above left - dotted- & right) if Mantik is correct. There is no such suture apparent. (A good copy of F8 shows this fairly clearly). |
|
 The fit of the bone on it's right border is also rather poor. The right border of the Harper fragment is concave - as is the bone against which Mantik would have us believe it fits. (above), This fact is somewhat neatly elided in his diagram (right, above). |
Mantik:
In particular; I wanted to know how far it would extend towards the right, because
the pathologists had placed their entry hole to the right of midline. As I measured this distance on F8 and compared
it to the well-defined distance along the bottom edge of the Harper fragment, I realized that the right edge of
the Harper fragment lay very close to the pathologists' EOP entry hole. But then it really hit me: after all of
this, I had quite unexpectedly placed the lead debris (on the Harper fragment, described by the Dallas pathologists
as possibly from a bullet, and still visible in the photograph) almost exactly where the pathologists had said
the bullet had entered. I stared, almost too shocked to believe it. I returned to the X-rays looking for possible
contradictions and found none. I reviewed all of the borders, to be sure that the X-rays permitted such a placement-and
they did! In addition, the lambdoid sutures, one on each side of the skull, as examined on both the lateral and
frontal X-rays, are also remarkably consistent with this interpretation.
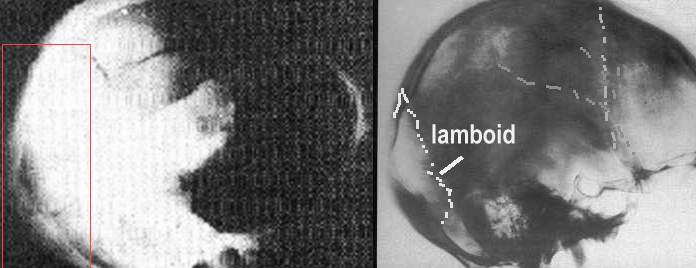
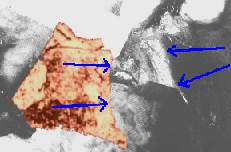
In fact the unenhanced autopsy lateral x-ray apparently shows no such large amount of missing occipital bone. (Above left, in red rectangle). It is hard to believe that Dr. Mantik found 'no contradictions' with this x-ray..The right hand x-ray above is JFK's (premortem) skull x-ray, with the suture lines marked. I have argued elsewhere that the right rear skull 'hole' seen at Parkland was in fact a large flap of skull & scalp hanging open there. (And Dr Mantik agrees that there was indeed a rear 'flap' of this kind.)

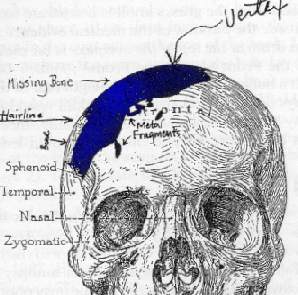
The large tendons of the neck attach at the nuchal lines, just beneath the fragment in Mantik's orientation. (The
'bar' like structure running across the skull beneath it, in the illustration above, from 'Murder In Dealey Plaza').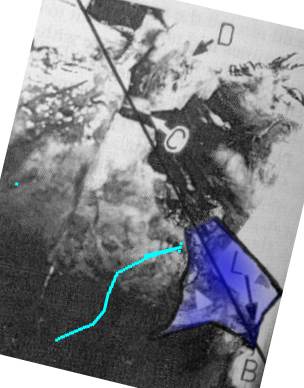
If Mantik's orietation is correct (above) these tendons seem to have been dissected away entirely. There are no
such things beneath the fragment (above).
Note also that almost the entire right side of the head is apparently missing - the red shaded area from the drawing
(above left) is not apparent (above). All that remains is a large flap of scalp.
The orientation cannot possibly be correct.
Mantik:
The Harper fragment (H) is shown situated in the occiput in Figure 2C. Letters C and
D identify bone fragments. Letter L denotes the site of lead on H. The 6.5 mm object is shown at about the 2 o'clock
direction from the right upper edge of H; it also lies directly inferior to the letter D. The letters McC (for
McClelland) identify the fi-acture that functioned as a hinge for a bone flap that could swing either open or closed.
This movement has been the cause of much confusion about the status of the occiput: when the flap was open (as
at Parkland) it produced an orange sized hole at the right ream; but when closed (as on the frontal X-ray) it seemed
that there was no major hole at the right rear. I have named this hinge after McClelland, who actually described
the bone flap. This fracture is also visible on the frontal X-ray. The area inferior to this flap is not well seen
on the X-rays (it is obscured by overlying hone), but the OD measure ments suggest that some bone is missing below
this flap. This would be consis tent with the eyewitnesses' recall of an orange-sized hole at this site. The semicirular
notch, located on line BA and just inferior to letter C, is where Baden placed the exit wound.
The Harper fragment (H) is placed into the frontal skull X-ray in Figure 2D. in this figure the lambda point (the
junction of the two lambdoid sutures and the saggital suture) lies slightly inferior to the top of the Harper fragment.
Most of the lambdoid sutures can he seen on the frontal and lateral X-rays, at sites that are consistent with this
interpretation. Furthermore, where these sutures are missing is exactly where the Harper fragment (not present
at the autopsy) fits into the skull. Optical density measurements confirm that bone is indeed miss ing where the
Harper fragment has been placed here. Baden's semicircular notch is not visible here, but must lie between bone
fragment C and the top of the Harper fragment. The letter L denotes lead on the Harper fragment. Regarding Baden's
notch, Roger McCarthy of Failure Analysis Associates has shown that beveling can occur from a gunshot even without
an exit or an entrance wound as the direct cause (Livingstone 1995, p. 313).
This is the simplest, and the most complete, integration of all of the known evidence. Furthermore, after looking
at genuine human skulls and textbooks, I see no real problem with the evidence on the bone itself, from either
the inside or the outside. Finally, though, I would emphasize that, like the certainty of the three autopsy pathologists
about the site of the entry wound, we should also take seriously the word of three Dallas pathologists who actually
saw the real 3D bone. They ali agreed that it was occipital, which is probably the best evidence we shall ever
get on this question. I have merely found the only reasonable place at the back of the skull where it could possibly
fit. Such a conclusion is, incidentally, yet one more proof that bone was indeed missing from the back of the head,
as if more proof were really required on this point.
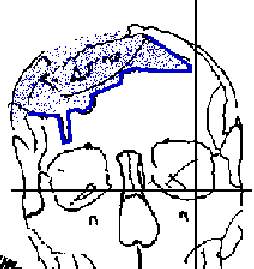 Angel |
 Mantik |
 Boswell |
"In order to approximate the position of the two major loose fragments it is neccessary to define the gap
seen in xrays (esp. 1& 2 & photographs esp. 44 trans & photograph.) of the head & skull
of JFK now kept at the National Archives." (Angel, report. Photo # 44 is the autopsy photo otherwise known
as 'F8', under discussion here). On this basis Angel produced the drawing (left, above). Mantik himself produced
the middle drawing above directly from the frontal x-ray. It is remarkably similar to Angel's. So also is Boswell's
drawing (right above) done at the autopsy (a top view, with the nose pointing down the page). Note the great &
absolutely obvious similarilty between Angels' drawing (based on F8) and Boswell's autopsy drawing (produced from
the body). Note the sharp 'notch' at the anatomical left of each picture. Note it also in F8, below, which actually
shows the forehead in the foreground with the scalp reflected down over the eyes. The blue line in all four pictures
(three above & F8 below) show the outline of the edge of the skull very roughly along the front hairline.
"... there should be no reasonable scientific doubt that the Harper fragment is, indeed, parietal bone"
(Riley)

{kind=link}